Misperception of biliary anatomy causes 71% to 97% of bile duct injuries. ICG-fluorescence imaging — sometimes called “the green light” — turns the unknown into something the surgical team can see in real time, before any cutting begins.
The Difference, Side by Side
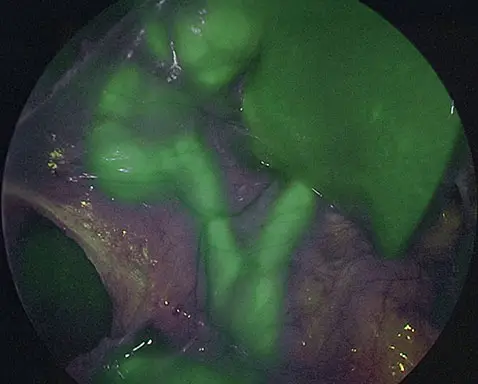
White light vs. Fluorescence-Guided Surgery
In conventional white-light laparoscopy the bile ducts blend into surrounding tissue. Indocyanine green (ICG) is a safe, FDA-approved dye that makes them glow under near-infrared light — the bright green you see when you drag the slider.
↔ Drag the handle. Real intraoperative footage — same procedure, same patient, two visualizations.)
0%
Reduction in BDI rates with ICG fluorescence imaging (Dip et al., meta-analysis, 2021)
0%
Relative increase in common bile duct visualization in a multi-center RCT (Dip, 2019)
0%
–
0%
Of all BDI involve the common bile duct — the structure ICG most improves
1
Inject
A small dose of ICG dye is given intravenously, typically 45 minutes before incision. The dye is excreted through the bile, concentrating in the biliary tree.
2
Illuminate
During laparoscopy the surgeon switches the camera to near-infrared mode. The ICG-saturated bile ducts fluoresce a bright green against surrounding tissue.
3
Identify
The surgeon achieves the “Critical View of Safety” with confidence — confirming the cystic duct and artery before any cutting or clipping.
How it works
Three steps, no incision change.
ICG fluorescence imaging adds about a minute to the standard cholecystectomy workflow. Most modern OR towers already support it — the question is whether your surgical team routinely uses it.
Why It Matters
Delayed recognition is the second tragedy.
Most bile duct injuries are diagnosed days to weeks after surgery — the bile leaks internally while the patient is sent home to recover. That delay is the single biggest predictor of serious complications, mortality, and successful malpractice claims.
4x
Higher 12-month mortality
The surgeon achieves the “Critical View of Safety” with confidence — confirming the cystic duct and artery before any cutting or clipping.
Booij, 2018; Tornqvist, 2012
#1
Reason for surgical malpractice
BDI is the most common cause of surgical malpractice litigation in the US. At least 1 in 2 BDI cases results in a lawsuit.
Hartnett, 2019
$10M
Recent verdict ceiling
2025 settlement awards reached $10M for a single plaintiff. Median ranges run $680K–$2.9M, with many cases exceeding $1M.
Hartnett, 2019; Wilsonlaw, 2025
Days → Weeks
Typical delay to diagnosis
Most BDI are diagnosed days to weeks after the original surgery — a delay strongly associated with morbidity and litigation.
Carroll, 1998; Ardito, 2023
Latest Research
New evidence on ICG fluorescence imaging for safer biliary navigation
A comprehensive review of 54 studies involving more than 3,000 patients explores how indocyanine green (ICG) fluorescence imaging can improve visualization of the bile ducts during cholecystectomy and help reduce the risk of bile duct injury.
We work with hospitals and training programs to make fluorescence-guided cholecystectomy the standard of care. If your facility has the tower and the dye, the only thing left is the protocol — and we can help you build it.
Of BDI caused by misperception of anatomy — exactly what ICG is designed to prevent
6 → 88%
Cystic-duct visibility before any cutting begins, with ICG vs. white light alone
Why It Matters
Bring this to your surgical consultation.
Most bile duct injuries are diagnosed days to weeks after surgery — the bile leaks internally while the patient is sent home to recover. That delay is the single biggest predictor of serious complications, mortality, and successful malpractice claims.